With MAID in mind
Exploring the accessibility and assumptions of medically assisted death in Western Canada


By Acacia Carol, Sarah Palmer, Bella Coco, Mia Smith
April 2026
Canada's medical assistance in dying (MAID) law is slated to include mental illness as a sole criterion come March 2027.
Since its February 2024 announcement, the federal government has left it to each region to assemble a course of action.
Ahead of the expansion, what is the current reality for patients seeking MAID, what do community leaders recommend should be considered, and how is Western Canada's healthcare system preparing?
Memoir: The reality of accessing MAID
How much is covered under the premise of reasonably foreseeable? What does compassionate expansion look like?


On April 21, 2020, in Lynn Headwaters Regional Park, British Columbia, as the rivers churned and spun, Donimo and her spouse, Sarah Leavitt, said goodbye to each other.
Donimo, a B.C. native, had come to the Headwater many times. Back then, her spouse, Leavitt, explains, Donimo had much greater physical mobility. She even had a large dog she would often take to the mountains or rivers.
Leavitt’s partner struggled with various complex medical conditions that often left her with chronic pain: myalgic encephalomyelitis (ME), postural orthostatic tachycardia syndrome (POTS), fibromyalgia, serious car accident injuries, and other conditions.
Despite years of various medical treatments to manage Donimo’s pain symptoms, in February of 2020, she was bed-bound and separated from the nature she enjoyed being a part of.
It was this escalation of excruciating pain symptoms that led Donimo to pursue medical assistance in dying, colloquially known as MAID.
In Canada, MAID recipients make up approximately five per cent of all deaths nationally. Legalized in 2016 after the Supreme Court unanimously ruled that the Criminal Code's prohibition on medical assistance in dying violated the Canadian Charter of Rights and Freedoms, MAID has been subject to various controversies, changes, and reviews at the provincial and federal levels.


Donimo and Jackson. Photo courtesy of Sarah Leavitt
Donimo and Jackson. Photo courtesy of Sarah Leavitt
Donimo and Jackson. Photo courtesy of Sarah Leavitt
Donimo and Jackson. Photo courtesy of Sarah Leavitt
Donimo and Jackson. Photo courtesy of Sarah Leavitt
Donimo and Jackson. Photo courtesy of Sarah Leavitt
Donimo and Jackson. Photo courtesy of Sarah Leavitt
Donimo and Jackson. Photo courtesy of Sarah Leavitt
Donimo and Jackson. Photo courtesy of Sarah Leavitt
Donimo and Jackson. Photo courtesy of Sarah Leavitt
Donimo's story
Before her application for MAID, Leavitt had seen Donimo pursue care through various channels, both traditional and alternative. A “pattern” Leavitt observed in her spouse’s complex medical case was that many treatments often didn’t work for Donimo, leaving some healthcare professionals “annoyed.”
It was during one of these hospital stays that the goal of Donimo's treatment changed.
“When she was at the hospital, she started saying, ‘I don't think I can do this anymore,” Leavitt explains.
The line between suicidality and the desire for a peaceful way to die was blurred, especially since Donimo didn’t believe she met the criteria for MAID. Leavitt said her partner ended up reaching out to a friend to research methods of ending her life.
“She ended up saying to Donimo, ‘the only way you can really guarantee that you're going to die is to take an overdose, but also put a plastic bag over your head,’” said Leavitt. “I would have had to leave the house so that no one would accuse me of being complicit in her death.”
The scene would have been traumatizing for her partner to come home to, Donimo had decided.
Suicide was not an option.

Artwork courtesy of Sarah Leavitt, Something Not Nothing.
Artwork courtesy of Sarah Leavitt, Something Not Nothing.
Despite doubts that Donimo would fit the criteria, Leavitt then contacted the province’s MAID care coordination office to inquire about the process.
Donimo was informed that she could submit an application. But that was only the beginning of her journey to receive MAID.

Artwork courtesy of Sarah Leavitt, Something Not Nothing.
Artwork courtesy of Sarah Leavitt, Something Not Nothing.


MAID and suicide
Arthur Schafer, the founding director of the Centre for Professional and Applied Ethics at the University of Manitoba, was a member of the provincial and territorial expert panel that helped establish the initial regulations for MAID.
Prior to 1972, when Canada decriminalized suicide, he said, a person could be persecuted for attempting to end their own life. Then, while suicide was legal for the sole person attempting, any person assisting, regardless of motives, could be guilty of murder or manslaughter.
In 2016, the Supreme Court suggested that regulations on physician-assisted suicide needed a few key eligibility criteria for patients to pursue MAID. A patient with a grievous and irremediable medical condition must be over 18 years of age, have the capacity to give informed consent, and make the request uncoerced in order to have assistance with their death.
Before the regulations were passed, then minister of justice, Jody Wilson-Raybould, added an additional requirement that the patient's natural death had to be reasonably foreseeable.
That language is vague, Schafer states, especially when compared to more solid criteria in other countries, where death must be determined within a specific time frame.

Artwork courtesy of Sarah Leavitt, Something Not Nothing.
Artwork courtesy of Sarah Leavitt, Something Not Nothing.
“What if I have a disease that will kill me, but may not kill me for a year, two years, three years? Am I eligible for MAID?” Schafer asks. “Do I have to be dying imminently?"
Reasonably foreseeable—two words that sparked significant struggle for a subset of patients who pursued MAID, patients with chronic illness. Patients like Donimo, who could continue to receive treatment and live, but face reduced ability in their day-to-day lives.
Donimo was a very active person who enjoyed the outdoors, Leavitt said. But in early 2020, she was unable to walk more than a few feet. Leavitt described that Donimo was often in intense pain, unable to move or speak.
A complicated healthcare system
Enter Bill C7, which was legalized in 2021 and created a two-track system of MAID eligibility. If a patient meets all the previously mentioned eligibility criteria but does not have a foreseeable death, they are on Track Two.
Sally Thorne, professor emeritus at the University of British Columbia, has been researching Track Two patients before there was even an official name for such cases.
“The systems involved in the support for those individuals who are likely going forward for Track Two is not nearly the same.”
Thorne believes that the general systems of support for patients with chronic illness, disabilities, or mental illness aren’t as robust as they should be. While it could get better, Thorne said, should patients seeking out better support have to wait until the system improves?
Waiting for the medical system to be better for patients also creates duress for medical practitioners. In her research, Thorne has observed a hesitancy from medical practitioners when a medically complex patient wishes to pursue MAID.
“It really does need to be a protracted, thoughtful process,” Thorne explained. “What we understand from having engaged with assessors over a large period of time is that so many of them go above and beyond in really trying to figure out how to identify any potential services that a person could have access to that they might not have been aware of.”
Chronic cases are often the most complicated for clinicians, she continues. When a disease has a known trajectory, practitioners can determine how care can change and evolve. But chronic illnesses can be different depending on each individual patient, making diagnosis and timelines more complicated.
“Some are in situations in which they don't have a diagnosed condition,” said Thorne. “They don't fit into a neatly packaged disease category.”
Adding MAID into the picture complicates things even more. Especially when these patients are on Track Two.
Clinicians often proceed cautiously in these cases, seeking additional consultation or obtaining opinions from multiple medical practitioners to ensure the patient receives the care they desire while still meeting legal eligibility criteria.
While that caution is crucial for practitioners, patients who have struggled to access treatment for their chronic issues in the conventional healthcare system are often frustrated by long wait times, continual testing, and sometimes physical symptoms. That frustration extends into similar issues when pursuing MAID.
For patients who struggle with chronic pain that is treatment-resistant, delaying access to MAID often comes at a high physical cost.


Eyes forward, chest up
Donimo herself faced many complications when pursuing MAID, Leavitt explains. Track Two did not exist yet, meaning that Donimo’s application would only be accepted if her death was considered reasonably foreseeable.
The first doctor who assessed Donimo determined that her death was not reasonably foreseeable and refused to approve her application.
The next doctor approved her application because she could see that Donimo had tried all possible treatments and that her life had become unbearable, with no possibility of relief.
It took some time to find a second doctor to approve the application. One specialist who had worked with Donimo refused to support her application because of religious reasons, and wanted to reattempt treatments that had been unsuccessful in the past. She then referred Donimo to a palliative care doctor.
Eventually, a second doctor determined that Donimo met the eligibility criteria for MAID. Leavitt said that, in the beginning, Donimo decided to receive MAID two weeks after approval was granted in early April 2020.
“Only a few people knew,” said Leavitt. “Then I had to tell her family and close friends, which was very [painful].”
What followed was an outpouring of love from Donimo’s chosen family community, from emails to people bringing dinners, to a socially distanced neighbour playing her guitar under Donimo's window.
Leavitt said her partner realized she wanted more time to spend with her loved ones. The date for receiving MAID was moved back one more week.
“It was this very strange time where all these beautiful things [were] happening, the kind of love that people gave us was incredible,” she said. “But Donimo was in horrible pain, and she was crying a lot. She was crying out in pain.”
Leavitt said she was in awe of the bravery her partner embodied while pursuing MAID. Leavitt couldn't comprehend how her partner could approach her own death with strength.
“The day that she died, we went to the park. She was talking with our friends and even doing some smiling and laughing, and I just couldn't wrap my head around it,” Leavitt recalled.
This brings us back to that afternoon in Lynn Headwaters Regional Park, behind the information center. The headwaters were crashing, loud and rhythmic. Donimo had requested that each person present for her passing tie a string around her wrist.
Something to take with her when she died.
Donimo gave permission for a doctor to administer a lethal dosage. Leavitt held onto the leash of the dog they shared.
“The river was very present,” said Leavitt. “I still haven't looked at most of the photos from that day… My dad has said that he can't believe how happy she looks.”
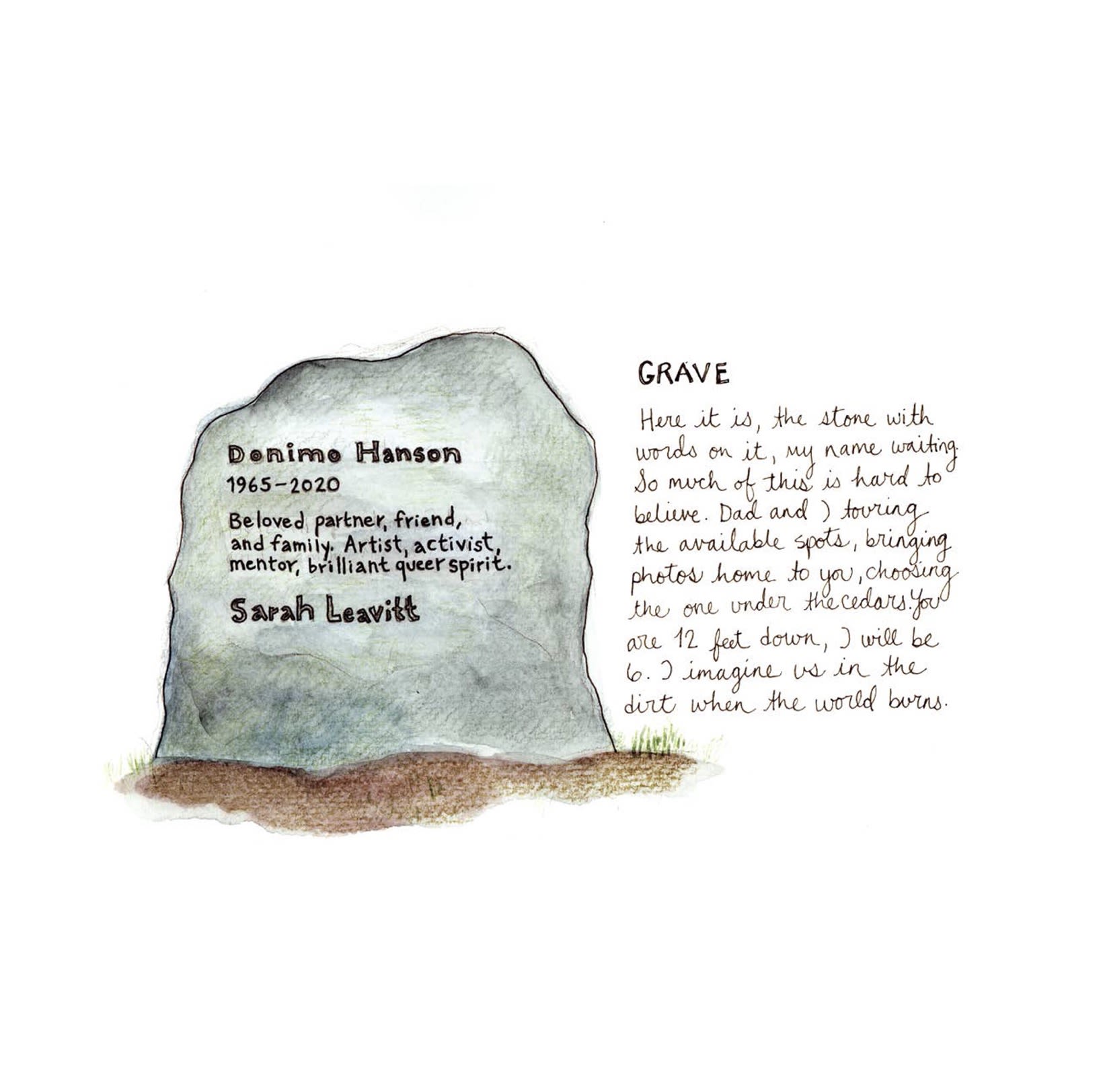
Donimo had a green burial and now rests beneath two cedars and a holly tree.

Artwork courtesy of Sarah Leavitt, Something Not Nothing.
Artwork courtesy of Sarah Leavitt, Something Not Nothing.
“There's photos of us looking down at the water, and I remember sitting by the water with her and our friend, asking if she felt ready,” Leavitt recalls. “They were talking about being ready to be part of nature. I think for her that [it] was very much about being part of the water and part of the plants.”


Donimo, Sarah, and their dog, Jackson at Lynn Canyon Headwaters. This was the area where Donimo received MAID. Photo courtesy of Sarah Leavitt
Donimo, Sarah, and their dog, Jackson at Lynn Canyon Headwaters. This was the area where Donimo received MAID. Photo courtesy of Sarah Leavitt


Creating something
After Donimo’s passing, Leavitt was thankful for the love she received from her queer chosen family. However, as grief so often does, she recalls the time after her spouse's passing as an “altered” state.


Artwork courtesy of Sarah Leavitt, Something Not Nothing.
Artwork courtesy of Sarah Leavitt, Something Not Nothing.
Keeping journals from this time, Leavitt used those entries to create a book about her experience with grief. Something, Not Nothing, was created during a time when she felt many conflicting emotions, like fear, sadness, and anger.

Artwork courtesy of Sarah Leavitt, Something Not Nothing.
Artwork courtesy of Sarah Leavitt, Something Not Nothing.
Still, out of her grief, she looks at the graphic novel created in that time of loss and grief with fondness.
“I often talk about it as my most joyful art experience. I haven't had anything like it since.”
Throughout this article, pieces of Something, Not Nothing, have been featured.

Artwork courtesy of Sarah Leavitt, Something Not Nothing.
Artwork courtesy of Sarah Leavitt, Something Not Nothing.


MAID changes
In the decade since MAID was legalized, major changes have fundamentally changed what palliative care could look like in Canada. But that’s not to say medical assistance in dying is without controversy.
MAID has faced opposition from religious groups since its legalization. Track Two was met with significant pushback from advocates for vulnerable populations, like those who live with disabilities or are unhoused.
Schafer explains that with the creation of Track Two, mental disorders as a sole underlying condition were specifically excluded. The inclusion of mental disorders was to be pushed back by two years in order to create effective guardrails.
“Two years went by, and the government said, ‘Oh, we’re not ready. We’ll still allow…it, but not for another year,’” Schafer said. “Then another year passed, and they said, ‘Not for another two years.’”
Even with these delays, federally, expansion for mental illness as a sole criterion will take place on March 17, 2027.
New Western legislation
Despite MAID being federally legislated, each province can set guardrails or guidelines regarding access to healthcare services.
This creates provincial differences in what pursuing MAID might look like for patients nationally. Quebec allows patients with a serious and incurable disease leading to incapacity to consent in advance to receiving MAID while they otherwise would not be fit to consent.
Currently, Bill 18, also known as the Safeguards for Last Resort Termination of Life Act, is a piece of legislation in Alberta that would impose limitations on MAID practices, including a prohibition on Track Two MAID.
The bill also prohibits medical assistance in dying for patients whose sole criterion is a mental illness, advance requests, and physicians from referring patients to pursue MAID eligibility assessments out of province.
Should Bill 18 pass, Alberta would be the only province with such legislated limitations on MAID.
During a March 18 press conference, Alberta Premier Danielle Smith said that the federal guardrails around MAID are “weakening” with the upcoming 2027 eligibility expansion.
Thorne, in a written statement following the press conference, believes that the bill does not take into account research, clinical knowledge and the experiences that have been documented throughout the last decade.
“It is highly concerning that Albertans are now being deprived of the autonomy other Canadians appreciate to be able to end their suffering and access end-of-life options,” Thorne wrote.


A bigger picture
Thorne believes that, for many Canadians, the debate and controversy over whether MAID should be an option have died down nationally.
“It exists, and therefore it's the health system's obligation to try and be sure we get it right,” she said.
To her, there are two primary ways that the current existing mental health system can compassionately support patients who wish to pursue MAID that respect their autonomy, while still protecting them.
First, Thorne believes that it is important to engage with a variety of mental health professionals, such as psychologists, clinical nurse specialists, and clinicians with expertise in specific mental illnesses.
Second, she believes that there needs to be a bigger push for a publicly funded mental health sector. Mental health, Thorne said, is not a special circumstance—it's a fundamental aspect of health.
Thorne is of the opinion that Track One should never be used as an alternative to high-quality palliative care, and Track Two cannot be used instead of investing in a robust public mental health and chronic health system.
She's also optimistic that Canadian health services can bridge that gap. In 2016, the conversation around palliative care was not nearly as involved with MAID as it is now. That barrier has been breached.
“We've got far more access to palliative care services and a palliative approach to care across community care and hospital care,” she said. “I think the consciousness about that has shifted, and hopefully systems are shifting in that direction.”
But how did we get here?
Past: Evolution of MAID
Taking a walk through the procedure’s progression in Canada


Like most things, medical assistance in dying (MAID) is not a new idea — rather, the modern label for a practice that is believed to have been around for a while. Namely, in a scholarly article by the University of Toronto’s Connor Brenna, MAID’s origins are dated back to the fifth century.
The following years saw many major religions speak out against euthanasia. From the Christian Bible to the Islamic Quran, the texts posit that “life was a trust from God, and to shorten or prolong it would interfere with God’s plan” since “artificially shortening life could preclude admission to the afterlife,” wrote Brenna.
Defining MAID
Some millennia later, when countries like Switzerland pioneered the decriminalization of medically induced death in the early 1940s, a new debate transpired under a familiar backdrop: what’s the difference between assisted suicide and euthanasia, who should have access, and is it ethical?
Assisted suicide
According to an article in the International Journal of Public Health, assisted suicide is when someone provides the information or means to help another person end their own life, including the prescription of drugs by a physician.
Euthanasia
Euthanasia, on the other hand, is the deliberate act of causing death to another person at their request.
MAID: Medical assistance in dying
By definition, MAID is Canada’s term for describing a form of euthanasia that is conducted by a physician who has followed the specific procedural safeguards outlined by their geopolitical location.
The terminology for MAID differs around the world, but as of 2020, medically assisted death, either self-administered or done by a clinician, is available to roughly 200 million people across Canada, Switzerland, and select parts of Australia, Europe, and the United States.
While Canada joins a few countries in having legalized MAID nationwide, the journey leading up to the 2015 decision resembled anything but a straight line. The debate began in the third quarter of the 20th century, and the decades that followed saw citizen advocacy culminating in political attempts that repeatedly fell through on Parliament Hill.
History of MAID in Canada

Photo by Raysonho on Wikimedia Commons
Photo by Raysonho on Wikimedia Commons
1970s to 1980s
Setting the stage
1972
Eighty years after it was first introduced in the Criminal Code, suicide was decriminalized in 1972. Similar attempts were made to do the same with assisted suicide, but these failed, and the procedure remained illegal.

Photo by Fotógrafo Samuel Cruz on Unsplash
Photo by Fotógrafo Samuel Cruz on Unsplash
1970s to 1980s
Early insight
1983
The Law Reform Commission of Canada recommended against legalizing euthanasia, saying that “aiding in suicide should not be decriminalized where assistance has been rendered to a terminally ill person.”


Photo by Kindel Media on Pexels
Photo by Kindel Media on Pexels
1970s to 1980s
Changing definitions
1987
Further amendments to the Criminal Code were made following even more recommendations by the Law Reform Commission of Canada, switching “mercy killing” from first-degree murder to being treated as second-degree murder — killing of another person that is not planned or premeditated.


Photo by @cdnhistoryexh on Instagram
Photo by @cdnhistoryexh on Instagram
Early 1990s
Meet Sue Rodriguez
December 9, 1992
Sue Rodriguez, a Canadian living in Victoria, B.C., diagnosed with Lou Gehrig’s, a fatal neurodegenerative disease more commonly known as amyotrophic lateral sclerosis (ALS), began her fight to overturn the law banning doctor-assisted death.

Photo screentshotted from Norma
Photo screentshotted from Norma
Early 1990s
Understanding the era
December 9, 1992
At that point, this was punishable by up to 14 years in prison under Section 241(b) of the Criminal Code. Rodriguez applied to the provincial Supreme Court to have the code amended, arguing that the law violated her rights under the Charter of Rights and Freedoms, but lost the case shortly after.


Svend Robinson (middle) in 2026. Photo by @karinagould on Instagram
Svend Robinson (middle) in 2026. Photo by @karinagould on Instagram
Early 1990s
Rodriguez's fight for change
December 29, 1992
Weeks later, New Democratic Party MP for B.C.’s Burnaby-Kingsway, Svend Robinson, introduced Bill C-385 to “allow for physician-assisted suicide upon the request of a terminally ill person.”

Screenshot of the 1993 appeal document. Photo by the Supreme Court of Canada
Screenshot of the 1993 appeal document. Photo by the Supreme Court of Canada
Early 1990s
Taking the fight higher
1993
Rodriguez took her fight higher, seeking to have the same section of the code overturned by the Supreme Court of Canada.
According to court documents, at 42 years old, she described her condition as “rapidly deteriorating” and that “she will soon lose the ability to swallow, speak, walk and move her body without assistance.”
On Sept. 30, 1993, judges sided with the code and found that Rodriguez’s application did not constitute a violation. Despite this, the split 5-4 decision suggested a shift in support for the decriminalization of physician-assisted suicide.


Photo by @cdnhistoryexh on Instagram
Photo by @cdnhistoryexh on Instagram
Early 1990s
Death highlights demand
1994
Rodriguez died at home with the illegal assistance of an unknown doctor on Feb. 12, 1994.
Supposedly, in response to her death, then Justice Minister Allan Rock stated that the process and treatment of suicide should not be a matter for parliament to decide. Later that month, a committee was formed to examine the social and ethical issues relating to euthanasia and assisted suicide.

Photo screenshotted from an archived Senate of Canada website.
Photo screenshotted from an archived Senate of Canada website.
Mid-1990s
Further discussions sparked
1995
The committee, called the Special Senate Committee on Euthanasia and Assisted Suicide, published its first report in 1995, titled Of Life and Death. Although the report, though the first of its kind, failed to reach consensus, it sparked further discussion on the quality of palliative care available to Canadians.

Photo by Welcome Collections Gallery on Wikimedia Commons
Photo by Welcome Collections Gallery on Wikimedia Commons
Mid-1990s
Legal questions raised
1998
A couple of years later, Quebec-based doctor Maurice Genereux became the first person sentenced under the law banning physician-assisted death. The ruling came after Genereux prescribed a lethal dose of barbiturates to two men diagnosed with depression and AIDS, with one of the men surviving the incident. Neither case was considered terminally ill.

Photo courtesy of amazon.ca
Photo by www.kaboompics.com on Pexels
Mid-1990s
Political momentum builds
1999
Sen. Sharon Carstairs introduced an act to facilitate decision-making about life-sustaining treatments and pain control. Named the Standing Senate Committee on Legal and Constitutional Affairs, the act failed to pass before parliament dissolved in 2000.

Photo screenshotted from Parliament of Canada
Photo screenshotted from Parliament of Canada
Turn of the 21st
Push for private bill
2005
Likewise, Quebec MP Francine Lalonde introduced Bill C-407, a private member’s bill which died at the dissolution of parliament that November. If passed, the bill would have permitted medical professionals to perform assisted suicide on a terminally ill person when deemed mentally competent at their request to die.


Photo by Tomi Blasic on Unsplash
Photo by Tomi Blasic on Unsplash
Turn of the 21st
Reluctant to lay charges
June 8, 2007
Two years later, a Canadian with multiple sclerosis, Elizabeth MacDonald, 38, died in Zurich with the assistance of Dignitas, a non-profit physician-assisted suicide clinic in Switzerland.
That July, the RCMP decided not to lay charges against her husband, who had accompanied Elizabeth on her travels and was with her at the time of her death.

Turn of the 21st
Convictions highlight grey area
June 12, 2007
Remesh Kumar Sharma, a physician based in Vernon, B.C., got handed a conditional sentence and had his license revoked after prescribing a lethal dose of drugs to a 93-year-old suffering from heart problems.
2008
Quebec resident Stephan Dufour became the first Canadian to stand trial by jury for assisting in the suicide of his uncle, whom he provided the means for doing so in September 2006. Dufour was acquitted by a Quebec jury, noting him as having a “limited mental capacity.”
2010
On the same note, an Ontario man, Peter Fonteece, pleaded guilty to criminal negligence two years later after not interfering with his “severely depressed” wife, Yansia’s, pursuit of suicide. He was later found not guilty.


Photo by @cbcfifth on Instagram
Photo by @cbcfifth on Instagram
Early 2010s
More hearings happen
2012
Like Rodriguez, the B.C. Supreme Court heard Gloria Taylor’s — another resident diagnosed with ALS — application to overturn the code, but it was later declared invalid.
That March, Quebec’s committee on Dying with Dignity tabled its report recommending legislative reform to facilitate euthanasia.

Photo screenshotted from Vlex
Photo screenshotted from Vlex
Early 2010s
Patterns are recognized
2013
In January, an expert panel based in Quebec recommended including euthanasia as a valid form of end-of-life care in provincial health legislation.
Change was pursued out West that October, as B.C.’s Court of Appeal overturned the judge's decision in Carter v. Canada, which had originally ruled that the Criminal Code was consistent with the Rodriguez case.


Photo by Wally Gobetz on Flickr
Photo by Wally Gobetz on Flickr
Early 2010s
Setting precedent
June 2014
One year later, Quebec became the first province to legalize MAID in 2014 for adult patients diagnosed with incurable illnesses, setting a precedent for future unravelings of the procedure’s criminalization.

Early 2010s
Euthanasia support grows
August 2014
An online poll conducted between Aug. 21 and 29 by Dying with Dignity and Ipsos found that 84 per cent of Canadians supported medical assistance in dying, stating that they agreed that “a doctor should be able to help someone end their life if that individual is a competent adult who is terminally ill, suffering unbearably and repeatedly asks for assistance to die.”

Photo by Jon Kolbert on Wikimedia Commons
Photo by Jon Kolbert on Wikimedia Commons
Legalizing MAID
Supreme Court ruling
2015
Assisted suicide, as done by a physician, is legalized after the Supreme Court voted unanimously on Feb. 6, 2015. The decision followed the agreement that the Criminal Code’s prohibition of the procedure breached constitutional rights, including a person’s life, liberty, and security, as listed in Section 7 of the Charter.


Photo by Antoni Shkraba Studio on Pexels
Photo by Antoni Shkraba Studio on Pexels
Legalizing MAID
Defining criteria
2016
One year after the Supreme Court decision, the federal government passed legislation establishing the criteria and procedural safeguards for medically assisted suicide, including that a person must be over the age of 18 and have an irremediable medical condition where natural death is reasonably foreseeable.
Photo by World Economic Forum on Flickr
Photo by World Economic Forum on Flickr
Legalizing MAID
Updating criteria
2019
The Superior Court of Quebec ruled the criterion that someone seeking MAID must have a reasonably foreseeable death as unconstitutional — prompting then prime minister Justin Trudeau’s Liberal government to propose expanding this by putting forward Bill C-7.

Photo screenshotted from Parliament of Canada
Photo screenshotted from Parliament of Canada
Legalizing MAID
Opening doors
2021
The bill was passed by parliament and approved by the senate in 2021, consequently removing a person’s reasonably foreseeable death as a mandatory criterion for obtaining the procedure. This opened the door to debates on the inclusion of psychological conditions.
Transitioning to today
By 2022, the fourth annual report on MAID in Canada detailed that medically assisted deaths accounted for four per cent of all deaths. The following annual report found that these deaths grew by almost 16 per cent in 2023.
Bringing us up to date, Bill C-62 came into effect in February 2024, officially temporarily delaying the expansion of MAID for people suffering solely from mental illness.
Today, Alberta and Western Canada are evidence of unique landscapes marrying the conflicting themes of community and separation — whether politically, financially, socially, or spiritually.
Ahead of the 2027 inclusion of mental illness as a sole criterion for obtaining MAID, how do the varying groups calling here home feel about the topic, and what do they recommend be done to ease the transition?
Present: Balancing beliefs
Exploring the convergence of spirituality and religion with MAID


In hospital rooms, homes and places of worship across Canada, conversations about death are increasingly shaped by a question that sits in the middle of medicine, law and faith: what role should spirituality play when someone is considering medical assistance in dying (MAID)?
Nearly a decade after MAID was legalized in Canada, the policy has become part of the country’s health-care landscape. Recent federal data show the number of assisted deaths rose steadily in the years following legalization before recent eligibility changes slowed the pace of expansion in 2023.


Photo by Leeloo The First on Pexels
Photo by Leeloo The First on Pexels


Photo by Igor Kyryliuk & Tetiana Kravchenko on Unsplash
Photo by Igor Kyryliuk & Tetiana Kravchenko on Unsplash
Even so, the practice continues to raise highly personal questions for patients and families managing the final stages of life.
For many people, those questions surpass medical eligibility or legal criteria. Topics such as suffering, dignity, and crossing faith teachings come into play, making the issue much more controversial.
In Calgary, conversations about MAID are unfolding across a range of spiritual traditions and groups.
A senior rabbi describes accompanying members of his congregation as they contend with the decision. A Mount Royal University (MRU) scholar draws attention to the broader health disparities Indigenous communities face in Canada. A Catholic bishop reflects on providing compassion with recommendations for alternative care.
Together, these perspectives illustrate how debates concerning assisted dying are not only legal or medical questions, but spiritual ones as well.
Jewish perspectives: Tradition, law and pastoral care
For Rabbi Russell Jayne, conversations about medical assistance in dying often begin with a difficult balance between religious teaching and the realities families face at the end of life.
Jewish tradition, he said, has long held that life and death ultimately belong to the divine.
“When I have been approached, I always talk about the fact that Judaism as a tradition does not support MAID because the mechanisms of life and death are in the hands of the divine,” Jayne said. “We are not allowed in any way to interfere with those mechanisms.”

While acknowledging Jewish tradition and rules, Jayne has also pushed to understand those seeking to use MAID. Photo by Acacia Carol
At the same time, he said his role as a rabbi does not end with stating the tradition’s position. When someone has already decided to pursue MAID, Jayne sees his own responsibility shifting toward pastoral care for the person and their family.
“For myself, I think that this is a bigger issue than whether or not I formally approve of the process,” Jayne said. “There’s the family, the loved ones, people that they’re leaving behind … they’re in a state of confusion.”
Jayne said he tries to be honest about the teachings of Judaism while also listening to the personal circumstances that led someone to consider assisted dying.
“I need to be honest with them about the tradition and about what the tradition accepts,” he said. “But I also have to be honest with their own particular journey and not belittle them and not belittle the process they have gone through.”
Within Judaism, Jayne emphasised, there is no one response among rabbis about how to handle situations like this. Some clergy choose not to be involved in MAID at all, while others take a pastoral approach similar to his.
“I have colleagues who are much more strict about the process than I am,” he said. “And I respect my colleagues who are anywhere on the spectrum.”
A covenant located at Beth Tzedec Congregation in Calgary. Photo by Acacia Carol
Jayne said those differences reflect the complexity of balancing religious law with pastoral care.
“This is something that is so challenging to deal with,” he said, adding that many rabbis wrestle with the same question: how to honour Jewish teachings while still supporting people facing the end of their lives.
Canada’s legalisation of MAID in 2016 has also shifted the conversations he has with congregants. Jayne said that before the law changed, rabbis could cite both religious teaching and legal restrictions. Now, he’s lost the ability to reiterate that medically assisted death is against the law.
That shift has reinforced his sense that his role is to clearly explain the tradition while recognizing that individuals may still reach their own decisions.
“You have a tradition that speaks against it, but you have the legal status of the procedure in the land,” he said. “That’s a great tension.”
In some cases, Jayne has been asked to be present when someone undergoes the procedure. For each case, the process has been performed in the individual's home rather than at a facility.
When the procedure happens, he said his role is primarily to listen.
From experience, he recalled arriving before the medical team and sitting with the family as they spoke about what they were feeling.
“Most family members would just talk to me and tell me practically anything about how they were feeling,” he said. “Most of them were not so much concerned about what they were feeling at the moment, but again, what exactly do they do once it’s finished?”

Beth Tzedec Congregation is known as Calgary's largest centre for Jewish life. Photo by Acacia Carol
Families sometimes ask him to incorporate elements of Jewish ritual or prayer. Other times, they simply want him nearby.
“Some families have asked me to sing songs from the tradition. Some people have asked me to recite psalms. Some people have asked me to do nothing,” he said. “But just knowing that I was there…that was very important to them.”
After the death, Jayne often helps guide overwhelmed families through the immediate religious practices surrounding burial.
“To have me there as a source of comfort, authority and direction, it has helped them quite a lot,” he said.
A common concern, he added, is whether their loved one will still be buried in a Jewish cemetery—something that carries deep significance in the community.


Beth Tzedec Congregation has been a part of Calgary since 1986. Photo by Acacia Carol
“We want to make sure that at that moment we are respecting the life of the deceased, giving comfort to the family and making sure that they understand that their loved one will be laid to rest with honour and with dignity,” he said.
For Jayne, being present during a MAID procedure can carry emotional weight, but he said he believes it is important that families do not feel abandoned by their faith at a time of grief.
“I cannot abide—no matter what I may personally feel—I cannot abide the thought that someone would think that at that moment of such hurt and loss and trauma that their religious tradition would abandon them,” he said.

While a place for Jewish faith and worship, Beth Tzedec Congregation also hosts the Calgary Interfaith Council and the Habitat for Humanity Interfaith Build Project. Photo by Acacia Carol
At the end of life, Jayne said, the focus is less on theological debates and more on making sure the person who has died and the family left behind are treated with dignity.
“Every human life is so precious,” he said. “We want to make sure that ultimately a person’s life is celebrated and that they are laid to rest with honour and dignity.”



Indigenous perspectives: Systemic health inequities
Anishinaabe scholar and MRU professor, Karen Pheasant-Neganigwane, said discussions about death and end-of-life care often start with the broader health disparities Indigenous people in Canada experience, with assisted dying being inseparable from the structural factors influencing Indigenous health.
Speaking about her own family’s experience caring for an ageing parent, she described how chronic illness is a common reality for many Indigenous families.
“My mom is needing 24-seven medical care, so that is why she’s in a nursing home,” she said. “The doctor has told me everything is slowly shutting down on her.”
Pheasant-Neganigwane explained that these experiences often reflect deeper systemic issues that are seldom addressed in public health discussions.
“One of the questions I ask students is, ‘What’s the number one killer of Indigenous people?’” she said. “The standard response is alcoholism or maybe suicide, or maybe these days drugs. But no—the number one killer is diabetes.”
She added that heart disease is also prevalent, linking these illnesses to the long-term effects of colonization and changes in food systems.


Pheasant-Neganigwane engages with social justice through artistic spirit, such as dancing. Photo provided by Karen Pheasant-Neganigwane
Research on Indigenous health outcomes supports this broader context. A 2026 study in the Journal of Palliative Medicine found that Indigenous communities in Canada continue to face significant disparities in health care access and outcomes due to colonialism and systemic inequities.
The study highlights that colonial policies, systemic racism, and social determinants of health continue to shape Indigenous experiences in the health-care system, affecting trust and access to services, including end-of-life care.
These legacies include documented histories of coercive sterilizations, racially segregated “Indian hospitals,” and medical experimentation on Indigenous people. Such practices have contributed to ongoing mistrust of health institutions.
Pheasant-Neganigwane pointed to similar historical trauma in her own family’s memories of residential schools.
“My mom…she can’t eat cream of wheat because it reminds her of maggots,” she said. “They would just take the maggots off and eat the other parts of the food.”
She noted that such experiences continue to influence how many Indigenous families view health, ageing, and care.
According to Health Canada, with patient consent, practitioners must collect information on race, Indigenous identity, or disability to identify systemic or individual inequities in the delivery of MAID.


Pheasant-Neganigwane performing in Regina. Photo provided by Karen Pheasant-Neganigwane
However, the recent review notes that Indigenous perspectives remain largely absent from research and policy discussions on MAID, despite its increasing role in Canadian health care.
This gap raises concerns about whether end-of-life care systems adequately address Indigenous cultural needs and support community-based decision-making.
Researchers found that family involvement, traditional practices, and community presence are often central to Indigenous approaches to end-of-life care.
For example, one study cited in the review found that about 90 per cent of Indigenous families surveyed emphasized the importance of family and community participation in end-of-life decisions.
Pheasant-Neganigwane noted that these values are reflected in memories of earlier generations.


Pheasant-Neganigwane giving a speech as the DCD hall of fame inductee. Photo provided by Karen Pheasant-Neganigwane
“Back in the day, we would be leading a full, healthy life and being at home,” she said, recalling when family and community members often surrounded Elders.
Today, she said, many families must navigate ageing and illness within institutional health-care systems. For Pheasant-Neganigwane, those shifts illustrate why conversations about assisted dying must also grapple with broader questions of health equity and social justice.
“When we’re talking about death,” she said, “we have to look at the health crisis going on.”


Catholic perspectives on assisted dying
In the Roman Catholic Church, assisted dying has been a subject of sustained theological debate and ethical reflection.
While the Catholic tradition emphasises a message of compassion and care, the sanctity of human life and historical opposition to the practice lead many to see MAID as “morally unacceptable.”
In Calgary, the Roman Catholic Diocese oversees 10 Catholic healthcare centres spanning Southern Alberta, none of which will perform MAID.
Diocese of Calgary Bishop William McGrattan said conversations about MAID are becoming more common across the Roman Catholic Diocese of Calgary, reflecting a broader shift in Canada’s health-care and legal landscape.
“In a number of fronts…it has come up in their family and their parish situation,” McGrattan said, describing how parishioners, pastoral care workers and hospital chaplains have all raised questions about MAID in recent years.


In 2017, McGrattan was appointed the eighth bishop of the Diocese of Calgary. Photo provided by Wikipedia
Those conversations, he said, often begin with people trying to understand how Catholic teaching applies to complex end-of-life decisions.
When individuals or families approach him or other priests, McGrattan said the first step is to understand their circumstances. From there, he begins the discussion within Catholic teaching, which emphasises the essential value of life.
“We often say that human life is a gift,” McGrattan said. “God as creator gives us this gift…and we have this responsibility to ensure that gift is respected.”
McGrattan said that the responsibility Catholics hold extends from the conception of life to the end.
“It’s at the end [of life] to allow for natural death to take place, so that we don't hasten death, that we don't make that choice of freedom to show disrespect to the gift of life that is created and given to us by God. So it's in that context that we try and show them,” he said.
At the same time, McGrattan said those teachings are shared within a broader pastoral context that acknowledges suffering and the need for care.
“There are ways in which the community and families can support them,” he said, pointing to the role of pastoral care workers and the importance of accompaniment.
He also emphasised palliative care as a key alternative to assisted dying, describing it as a way to support people at the end of life without prolonging suffering.
“There are these specialised units where individuals and nurses allow people to experience natural death, but without pain. There is this comfort, and there is this understanding that they will not suffer unduly,” McGrattan said.
McGrattan also expressed concern about how eligibility for MAID has evolved over time, arguing that safeguards have weakened since the law was first introduced.
“The federal government has basically eroded those buffers to the point now that they're talking about those who have mental illness, some in social and living situations, who find it unbearable, can make a request,” he said.


In Alberta, he noted, there have been efforts to address those concerns at the provincial level.
On March 18, the Alberta government introduced Bill 18, the Safeguards for Last Resort Termination of Life Act. If passed, doctors and nurses could not administer MAID to patients with mental health as their sole condition for application.
In his conversations with parishioners, McGrattan said certain concerns recur, particularly fear of burdening others and uncertainty about end-of-life care.
“People often in advanced age find that they might be a burden,” he said. “Or people feel that they might be alone or that they might be abandoned at the end of their life."
He also pointed to what he described as misconceptions about pain management at the end of life.
“I think it's really about educating people that there are alternatives which respect human life and that people can seek and have access to in such situations,” McGrattan said.


McGrattan delivering his first homily as bishop. Photo provided by the Roman Catholic Diocese of Calgary/Victor Panlilo
While Catholic clergy may accompany individuals through illness and end-of-life insight, McGrattan said they do not attend the administration of MAID itself. In the faith, being present at the procedure is not the norm for Catholic clergy and would be seen as participating in the act.
“That would be considered to be an accomplice, and showing that they are somewhat supporting that by being very present,” McGrattan said.
Even so, he emphasised that pastoral care remains central before that point, with clergy offering support, conversation and guidance.
“It sounds like we're not being compassionate or considerate, but we want to walk with the person. We offer various conversations, counselling, and try to assist them to maybe see in the discernment and decision that there are alternatives,” he said.
More broadly, McGrattan said the growing acceptance of MAID raises wider questions about how society views those who may be at risk.
“I think sometimes we begin to wonder, you know, as society is making such choices, is there really a respect for human life? And then we can go through the whole gamut of our human experience, including people who are homeless, in need of food or shelter, or in need of medical care,” he said. “So I think the question is, how is society treating its most vulnerable?”
He linked those concerns to what he described as a broader cultural shift, referencing a phrase used by Pope Francis.


Pope Francis and Bishop McGrattan meeting in Rome during the 2017 Canadian Bishops' Ad Limina visit. Photo provided by the Roman Catholic Diocese of Calgary/L'Osservatore Romano
“He said, ‘We live in a society that is a throwaway culture,’ and this whole idea that even as we throw away things that we have, we shouldn't necessarily have that same attitude and approach to human life,” McGrattan said.
At the same time, he said discussions about MAID should include a range of perspectives, including those shaped by faith.
“What we would like to have is the ability to bring our faith, our convictions, and to be part of this discussion,” he said.


Faith, care and realities shaping end-of-life care
The Calgary Journal reached out to other faith leaders, but did not receive a response.
Across different traditions and experiences, conversations about MAID reveal that questions of death rarely exist in isolation from the broader contexts that shape people’s lives.
For some spiritual leaders, that means helping families navigate moments of grief while holding space for religious teachings that may not always align with personal decisions. For others, it means asking how systemic inequities shape the conditions under which those end-of-life decisions are made.
While MAID remains a legal option within Canada’s health-care system, the perspectives surrounding it continue to reflect deeply personal beliefs about dignity, suffering and responsibility at the end of life.
Future: What's next
With MAID's possible expansion, Canada faces tough questions about limits, safeguards, and who decides


For the past four decades, the Canadian government has wrestled with the legal inclusion of medical assistance in dying (MAID). But now, following the 2016 federal legalization, the government is slated to consider another major decision.
Come March 2027, the federal pause on allowing mental illness as a sole underlying condition for MAID is set to expire, bringing governments, physicians, and the public to confront the difficult question: should mental illness be allowed to be a sole criterion for MAID?
Since its federal legalization, MAID has expanded from a complex legal framework into a medical service that thousands of Canadians access each year.
Few onlookers have followed its legal and ethical evolution as closely as Rose Carter, an Edmonton-based health lawyer with more than 30 years of experience studying the issue.
Carter explained that MAID itself exists as an exception within the federal Criminal Code, allowing physicians and nurse practitioners to provide assisted death under very specific legal precautions.
Carter said that to understand what will happen this time next year, we need to understand the intricacies of how it works now.
As it stands today, Carter said three basic criteria must be met before someone can even begin a conversation about MAID. You need to be a citizen of Alberta, be a legal adult (at least 18 years old), and have legal capacity.
The concept of legal capacity can complicate the process. What does it actually mean to have full legal capacity?
In practice, two independent assessors must evaluate the person requesting MAID to determine whether they qualify and whether they are capable of making the decision. Those assessors must be satisfied that the patient understands what they are asking for and the consequences of that choice.
Carter compared the requirement to another familiar legal process.
“It’s no different than someone preparing a will,” she said. “You have to understand what you’re doing and the implications of the decision you’re making.”
In 2021, the federal government created an expert panel to which Carter was appointed to examine whether MAID should be allowed when mental illness is the sole underlying condition.
The panel’s 2022 report outlined a list of 19 recommendations covering a range of practice standards.
The panel decided that the 19 recommendations should be divided into five sections: MAID practice standards, the interpretation of “grievous and irredeemable medical condition,” vulnerabilities, the assessment process, and implementation.
This process is open to interpretation, as it does not mean the government must comply with the panel’s suggestions.
The recommendation suggests that, in cases of incurable conditions, both physicians and nurses should follow a framework consistent with existing MAID practices, including built-in safeguards.
According to the Government of Canada, a grievous and irremediable medical condition is not limited to terminal diagnoses, but also any serious illness, disease, or disability that is rapidly declining and incurable.
Together, the framework provides safeguards while allowing physicians and nurses to apply MAID thoughtfully and responsibly in cases involving mental illness.
Bill C-62, introduced in Feb. 2024, officially delayed the expansion of MAID to people suffering solely from mental illness until 2027.
As of March 16, 2026, the Alberta government released legislation that restricts access to MAID.
If enacted, the Safeguards for Last Resort Termination of Life Act would ban what is often called “Track 2” MAID cases where a person’s natural death is not reasonably foreseeable.
“MAID should not become a permanent response to a moment of crisis or despair,” said Smith on March 18, 2026, at a press conference in Edmonton.
Smith said the province’s approach reflects a position that MAID should remain limited to circumstances involving serious illness where recovery is not expected.
Alberta’s NDP will have to review the new legislation before taking a position.
At the announcement, Smith said the province has serious concerns about broadening eligibility to include mental illness, pointing in particular to issues related to cases where death is not reasonably foreseeable.
Ultimately, Carter said the debate over MAID and mental illness isn’t a straightforward yes-or-no issue, and it’s unlikely to have a clear-cut answer in the years ahead.
The scale of mental illness is still not identifiable, so that is where the question comes in: how do we identify what is constitutional?
Carter said accessing MAID for mental illness would likely be a long and complex process.
Patients would need to demonstrate a long history of mental illness and undergo multiple assessments, including evaluations by at least two psychiatrists.
However, she noted Canada already faces a shortage of psychiatrists, meaning access and timelines could depend heavily on specialist availability.
Because MAID is governed by the federal Criminal Code while health care is administered by the provinces, Carter said it remains difficult to predict exactly what the program will look like in Alberta in the coming years.
As the 2027 date approaches, the conversation surrounding MAID is likely to intensify. And while the future of the policy remains uncertain, Carter said one thing is clear: understanding how the system works today will shape how Canada decides where it goes next.
“It's going to be a long and torturous journey for patients,” said Carter.







{kind=link}
{kind=link}
{kind=link}

About us
Hello! Thank you for visiting
We are Calgary-based journalists who completed this project as part of a capstone course while in our 4th year of the Journalism and Digital Media program at Mount Royal University.

Acacia Carol
Lead Reporter

Sarah Palmer
Researcher & Data Visualizer

Bella Coco
Secondary Reporter
